
Politics of harm reduction: HIV outbreak in W.Va.’s capital shows police and politicians can’t replace doctors and public health experts
Despite warnings from multiple organizations, city officials ushered in the “most concerning outbreak in the nation” by pressuring the shutdown of the Kanawha Charleston Health Department syringe program. After five years of inaction, officials are voting to make any syringe program using the CDC’s recommended practices illegal.
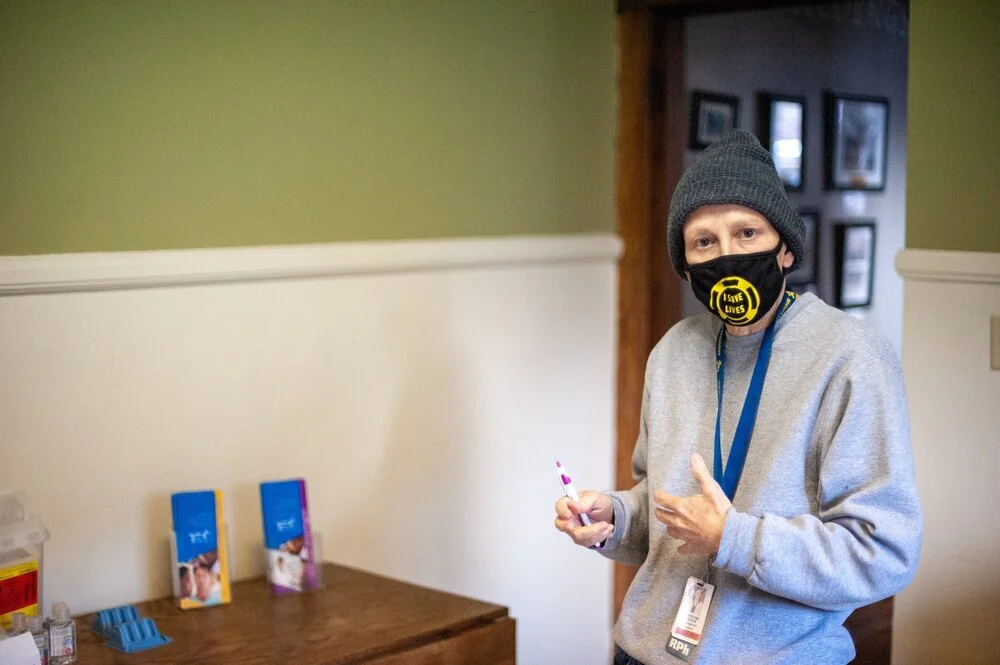
Dr. Teague uses a community-based harm reduction program to access at-risk populations for HIV testing in Charleston, W.Va. Feb. 20, 2021. (Photo/Kyle Vass)
Apr. 3, 2021 • Written by Kyle Vass; Edited by Lacey Johnson
Sign up for our newsletter to get all of our stories delivered to you as they happen.
CHARLESTON, W.Va. (Dragline)—Dr. Michael Brumage hasn’t slept well since 2018. The former director of the Kanawha Charleston Health Department says the rise in overdose deaths and new HIV infections that have occurred since the shutdown of the KCHD syringe program in Charleston, W.Va. haunt him to this day.
“People are literally dying because of this issue. This is what I have to live with day in and day out.”

Dr. Brumage started Charleston's first needs based syringe program in Charleston, W.Va. but was forced to close it down amid intense political pressure in 2018. (Photo/WVU)
Dr. Brumage served 25 years in the US Army as a physician and moved back to Charleston to take on what he called a “retirement job,” as director of the KCHD. He was excited to fight the opioid pandemic that had ravaged his home state. “That was going to be my retirement home. I planned to stay in Charleston for as long as I could.”
But, while Dr. Brumage was planning his homecoming, a new front was opening up in the battle against the opioid epidemic—outbreaks of HIV in rural communities from intravenous drug use. Dr. Brumage has just seen Austin, Indiana make headlines in 2016 when 235 people in a town of fewer than 5,000 were found to have contracted HIV associated with injecting drugs.
The outbreak was called “the worst drug-fueled HIV outbreak ever to hit rural America.” And as officials at the CDC researched the phenomena, they found Scott County was only the beginning.
Two hundred and twenty counties nationwide were identified by the CDC as high-risk for rural HIV outbreak related to injecting drugs. Kanawha County was on the list. Six years later, Kanawha County has surpassed the other 219 high-risk counties to become the site of the most concerning HIV outbreak in the nation according to the CDC.
After the CDC announced its list of 220 high-risk counties, Dr. Brumage took over as the director of the KCHD. He says in his first week on the job he was approached by Dr. Michael Kilkenny, the director of the Cabell Huntington Health Department, about starting a sterile syringe program. Cabell County, home to the state’s second largest city, Huntington, was also on the CDC’s list.

The Kanawha Charleston Health Department served over 3% of the population in Charleston, W.Va. before being forced to close down in 2018. (Photo/KCHD)
“They came over to tell us that they were going to start a syringe service program at the Cabell Huntington Health Department and that they would like to see something get started in Charleston at the same time, because they knew we were communities that were very close together with similar problems.”
Dr. Brumage said Dr. Kilkenny gave him permission to copy their plan for a syringe program word for word, and the two programs took off. Dr. Brumage’s program in Charleston saw the number of people visiting the KCHD go up by 15 new participants a week. But, unlike Huntington, Charleston’s mayor, Danny Jones, hated the idea of a syringe program—especially one operating across the street from where $100 million was being spent on renovating the city’s convention center.

The most recent renovations to Charleston Coliseum and Convention Center cost the city $100 million in 2019. (Photo/Kyle Vass)
The shutdown of the KCHD syringe program
The city had just begun renovating the convention center when the KCHD syringe program started to take off. At the time, Jones took to his own radio talk show to spread misinformation about harm reduction and call for an end to the KCHD syringe program. In one such interview, Jones made national headlines by referring to his own city’s health department as a “mini-mall for junkies.”
When Dr. Brumage spoke to Jones privately about his accusation, Jones said that it was the newly appointed chief of police, Sgt. Steven Cooper, who was driving the push to shut down the KCHD syringe program. Then in January 2018, a public relations nightmare struck when a small child stepped on a syringe in the bathroom of a fast food restaurant. The event prompted Sgt. Cooper to redesign the syringe program from the ground up, using powers granted by a municipal ordinance from 2015.
The new rules Sgt. Cooper set in place for the program included a strict “1 for 1” exchange model. People who fail to bring a single syringe back upon returning to get more would be kicked out of the program. But public health experts, including Dr. Brumage, knew that this model of syringe program was more likely to spread viral transmission.
“If you don’t want people sharing equipment, you have to give people adequate supplies so that they never have to share," said Terry Morris, director of the San Francisco Aids Foundation in a 2018 interview. "When people save their syringes for reuse, because of scarcity, they’re more likely to loan them to someone else. If they immediately throw used syringes into a bio-bin for disposal, because they’re not worried about scarcity, they’re going to be safer.”

Former Chief Steven Cooper retired from the Charleston Police Department months after the shutdown of the Kanawha Charleston Health Department Syringe Program in 2018. (Photo/Charleston Police Department)
Another rule put forth by Sgt. Cooper was that only single-use, retractable needles would be distributed. However, harm-reduction research has shown that retractable needles can spread both blood-borne viruses and bacterial infections. Introducing syringes that can’t be reused into a program, creates a scarcity of syringes and leads to dangerous work arounds by people who inject drugs. These retractable syringes can be shared for a moment before the needle retracts. People, faced with this scarcity, will also tamper with the retraction mechanism to modify the syringe into a reusable one and can contaminate an otherwise sterile syringe in the process.
The KCHD was faced with two options: modify Dr. Brumage’s successful syringe program in a way that would cause harm to the people who relied on it or shut it down completely. The health department chose the latter. A syringe program that had served 24,740 participants, including 3.8% of Charleston’s population, shut down overnight. Two months after its closure, the city's harm-reduction efforts would be dealt an even bigger blow.
Creating the myth of a “poorly run program”
Acting as the state’s top health official, Dr. Rahul Gupta authored a scathing report on the KCHD syringe program at the request of Mayor Jones, who said its participants “should be locked up until they’re clean.”
Gupta, who has been discussed as President Joe Biden’s most likely pick for drug czar, published the report just four months before resigning from his position. Unlike the criticism from law enforcement agencies and NIMBY politicians whose claims framed harm reduction as enabling drug use, Gupta’s report focused largely on the back end of the KCHD syringe program—namely, record keeping.
Gupta took issue with the fact that there weren’t complete datasets on how many syringes participants had been given and when. His report also criticized the KCHD syringe program for not insisting that participants be educated on drug recovery options prior to receiving syringes. The report also criticized the program for allowing people to pick up syringes for other people.
Despite the KCHD program already closing its doors, the thesis of Gupta’s report was that the program should not be allowed to operate. Public health experts around the nation submitted letters critical of Gupta’s report to the state health department.
None of Gupta’s findings were based on CDC guidelines for running a syringe program. However, the idea that the KCHD syringe program was poorly run has been echoed throughout Charleston by politicians and citizens, who are against following CDC recommendations for combating the current HIV crisis—specifically, opening syringe access to the community.

Dr. Rahul Gupta issued a report critical of the Kanawha Charleston Health Department syringe program four months before retiring as the state’s health officer. He’s now considered the lead choice for Joe Biden’s pending drug Czar appointment in 2021. (Photo/WVNews)
In an interview on the report, Gupta said that his report “should be a lesson for other needle exchanges in the area.” He resigned four months later. Within a year, a Cabell County commissioner used the report issued by Gupta to request that the state health department audit the Cabell Huntington Health Department syringe program. That request was denied, and the program that started in tandem with Brumage’s program has since been successful in turning the tide against HIV transmission in Cabell County.
Three years later, as Charleston finds itself facing the “most concerning HIV outbreak in the country,” the city council is using Dr. Gupta’s report to support a new bill that would make any program that operates under the CDC’s guidelines for syringe programs illegal. Council members will vote on this bill Monday.
The report is also being used to bolster a bill in the West Virginia Legislature that would shut down all syringe programs in the state. All, but perhaps one.
Elected officials who have tried to get syringe programs shut down in the state for years have held up West Virginia Health Right as having a superior syringe service program because it requires patients to adhere to a strict one for one exchange model. If patients fail to return their syringes to the clinic, they are kicked out of the program.
Harm reduction experts, however, have long known this model to be ineffective. Yet, having this rule is the only way for which staunch opponents of harm reduction like State Senator Eric Tarr, the author of the bill, tolerate having a sterile syringe program.
Though Sen. Tarr never mentioned West Virginia Health Right in this video he made explaining his harm reduction bill, he made reference to having spoken with the “operators of syringe program” that were “successful in getting a one to one exchange,” who used “serial codes on their syringes.” As West Virginia Health Right is the only syringe program in the state that uses barcodes on its syringes, that clinic was the standard used to write this bill.
But, West Virginia Health Right having the support of politicians who have fought for years to shut down syringe programs in the state (such as Cabell County Commissioner Kelli Sobonya and former Charleston Mayor Danny Jones) the clinic has been slammed by medical experts for creating a program that alienates people who use drugs and drives them away from the medical field as a whole.

Former Mayor Danny Jones hands a check to Angie Settle, the Director of West Virginia Health Right in 2018. Danny Jones was an ardent critic of the Kanawha Charleston Health Department syringe program and fought for years to get it shut down. (Photo/WV Metro News)
In a study published in The Harm Reduction Journal, medical experts spoke to former patients who attended West Virginia Health Right’s syringe program. Their experiences spoke of an environment of stigma and shame. The former patients, many of them unsheltered, cite this stigma and an inability to carry around a month’s supply of used needles as reasons they no longer went to the program.
“You know, they just make you feel really uncomfortable. They make you feel like you’re a bad person, like, you know what I mean?”
One former patient even described resorting to taking apart the retractable syringes they offered at the time (a practice since discontinued by the clinic)—a practice that experts have shown to be highly dangerous in contaminating otherwise sterile syringes.
“The ones [syringes] at the [clinic SSP] are retractable, one-time use. And it’s like, well, you cannot push them down all the way but then you’re not getting all your dope or… I mean, I’ve figured out where I can actually take the syringe apart and put it back together where it will retract but you know, that can be an ordeal sometimes especially when you’re on the streets.”
Despite Angie Settle, the director of West Virginia Health Right, being warned by multiple people (who have chosen to remain anonymous but supplied Dragline with proof) that giving retractable syringes was a dangerous practice, Settle was faced with pressure from the City of Charleston. At that time, the city had passed an ordinance adopting rules governing syringe programs written by then Chief of Police Steven Cooper. Cooper would retire in the following months and Settle’s clinic would go back to conventional syringes.
When the dust settled, the battle of two models for syringe programs, high vs. low barrier, had played out in Charleston. To this day, the only place for people who inject drugs to get syringes in the city is the clinic that “makes [drug users] feel like bad people.”
The battle in Charleston helped ushered in what the CDC has called the “most concerning HIV outbreak in the country.” With the passage of Sen. Eric Tarr’s bill, the entire state is on the threshold of seeing what happens when you lose harm reduction.